

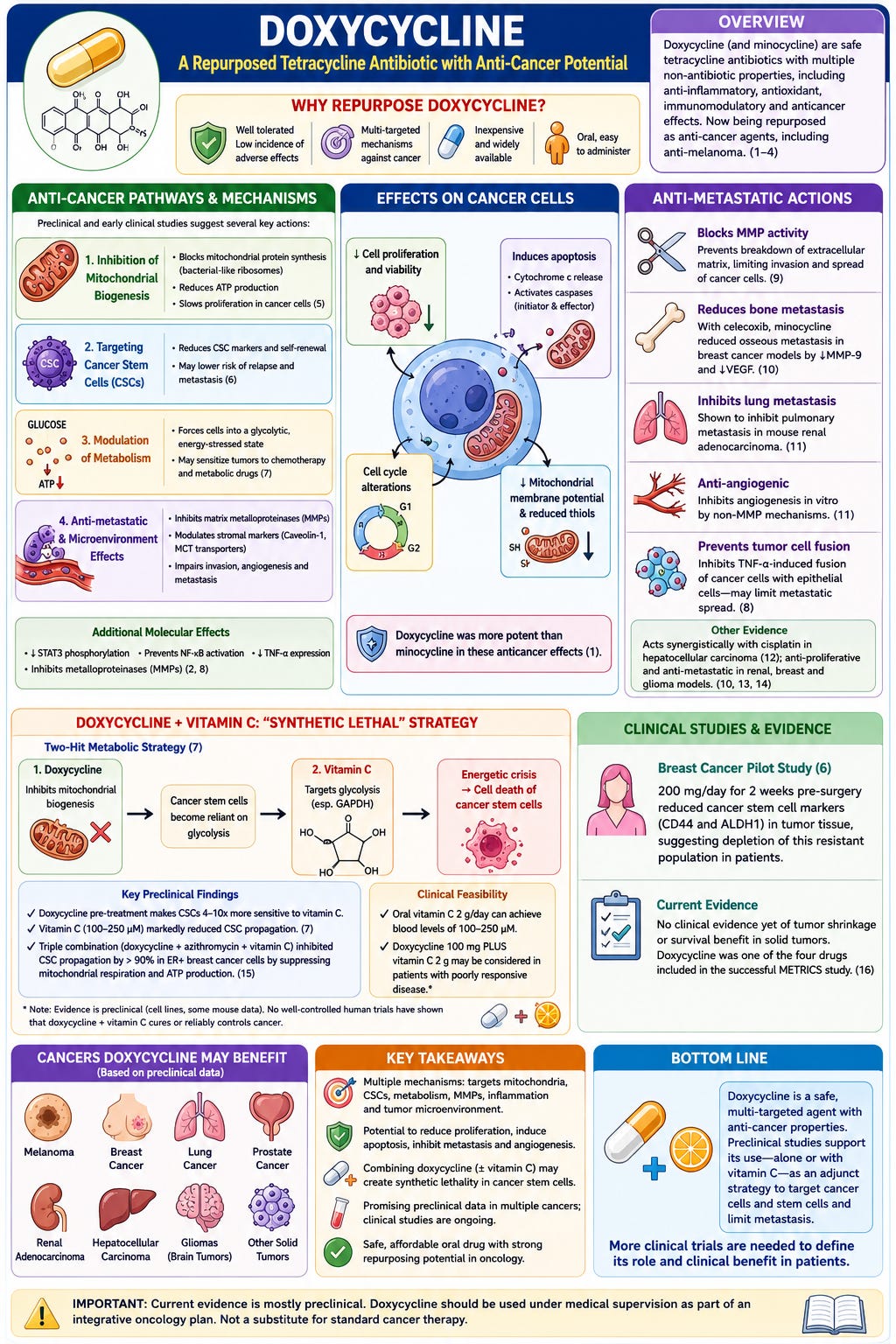
Doxycycline and minocycline were introduced into medicine as more potent, active, and stable semisynthetic tetracycline antibiotics. In general, the incidence of adverse effects caused by minocycline and doxycycline is very low. In addition, they show many non-antibiotic properties, including anti-inflammatory, antioxidant, neuroprotective, immunomodulatory, and anticancer effects. (1, 2) Recently published studies and analyses considered the repurposing of minocycline and doxycycline as anti-melanoma agents. (3, 4)
Anticancer pathways and mechanisms
Preclinical and early clinical work suggest several potential anti‑cancer actions (see Figure 1):
Inhibition of mitochondrial biogenesis: doxycycline blocks mitochondrial protein synthesis (because mitochondrial ribosomes resemble bacterial ribosomes), which can reduce ATP production and slow proliferation in various cancer cell lines.(5)
Targeting cancer stem cells (CSCs): multiple groups report that doxycycline reduces CSC markers and self‑renewal in breast and other cancer models, which could lower risk of relapse and metastasis.(6)
Modulation of metabolism: by forcing cells into a more glycolytic, energy‑stressed state, doxycycline may sensitize them to other therapies, including chemotherapy and metabolic drugs.(7)
Antimetastatic and microenvironment effects: doxycycline can inhibit matrix metalloproteinases and appears to affect stromal markers such as Caveolin‑1 and MCT transporters that are linked to tumor progression.
Figure 1. Anticancer pathways of Doxycycline
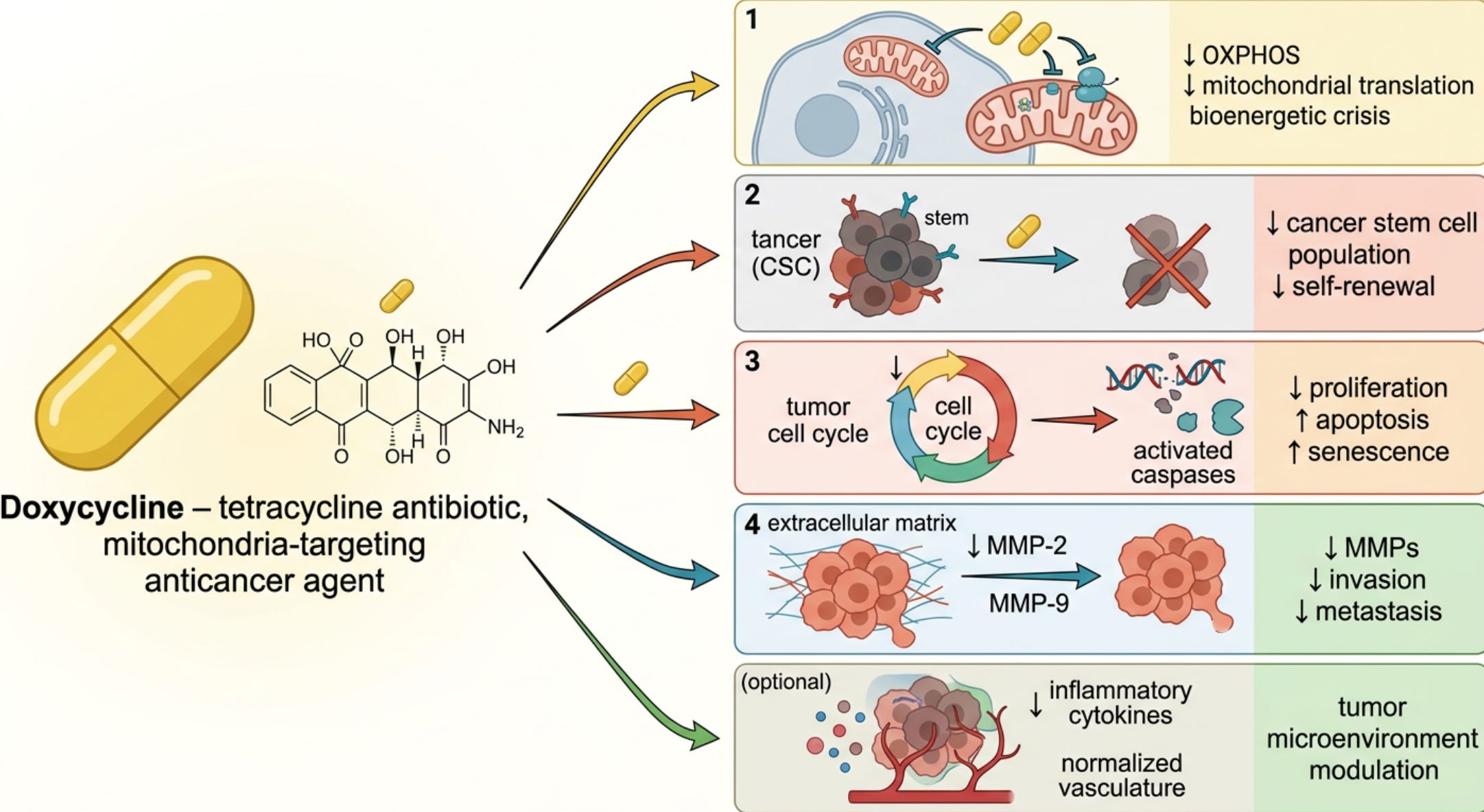
Mechanisms of the anticancer activity of doxycycline and minocycline involve reduction of STAT3 phosphorylation, prevention of NF-ΚB activation, repression of tumor necrosis factor (TNF) - α expression and inhibition of matrix metalloproteinases. (2, 8) Minocycline and doxycycline have been demonstrated to exert anti-melanoma effects. (3, 4) These drugs inhibited cell proliferation, decreased cell viability, and induced apoptosis. Rok et al demonstrated similar findings in amelanotic melanoma cells. (1) In this study, the treatment caused changes in the cell cycle profile and decreased the intracellular level of reduced thiols and mitochondrial membrane potential. In addition, exposure of melanoma cells to minocycline and doxycycline triggered the release of cytochrome c and activated initiator and effector caspases. In this study, doxycycline was a more potent drug than minocycline in mediating these anticancer effects.
Doxycycline blocks the activity of metalloproteinases, which would otherwise be involved in the breakdown of the extracellular matrix that allows individual cancer cells to break free and seed new metastatic cancer growth around the body. Considering the potent inhibitory effects of tetracyclines against metalloproteinases, their anticancer potential has been studied in a variety of cancers, including melanoma, lung, breast, and prostate cancers. (9) When combined with celecoxib, minocycline inhibited the osseous metastasis of breast cancer in nude (hairless) mice, by increasing tumor cell death and decreasing tumor expression of MMP-9 and VEGF. (10) Minocycline has been shown to inhibit in vitro invasion and experimental pulmonary metastasis in mouse renal adenocarcinoma. In addition, these drugs have been demonstrated to inhibit angiogenesis in vitro by a non-metalloproteinase-dependent mechanism. (11)
Weiler et al demonstrated that minocycline inhibited the TNF-α-induced fusion of cancer cells with breast epithelial cells; (8) this may have an important role in limited metastatic cancer spread. Minocycline has been demonstrated to act synergistically with cisplatin in the treatment of hepatocellular carcinoma. (12) Anti-proliferative and anti-metastatic properties of minocycline have also been demonstrated in various other types of cancer, including renal adenocarcinoma, (13) breast cancer, (10) and malignant gliomas. (14)
Doxycycline + vitamin C combination (“synthetic lethal” idea)
A key lab paper proposed a two‑hit “metabolic” strategy: doxycycline first forces cancer stem cells to rely almost entirely on glycolysis by inhibiting mitochondrial biogenesis, then vitamin C targets glycolysis (especially GAPDH), leading to an energetic crisis and death of these cells.(7) In cell culture, cancer stem cells pretreated with doxycycline became 4–10 times more sensitive to vitamin C; vitamin C at 100–250 μM markedly reduced their ability to propagate.(7) Another in‑vitro study found that a triple combination of doxycycline, azithromycin, and vitamin C inhibited CSC propagation by more than 90% in an ER‑positive breast cancer cell line, mainly by suppressing mitochondrial respiration and ATP production.(15) These findings are all preclinical (cell lines, some mouse data), and there are currently no well‑controlled human trials showing that doxycycline plus vitamin C cure or reliably control cancer. This approach does appear to be clinically feasible as a1- 2g dose of oral vitamin C would achieve the blood levels (100-250 uM) required for this interaction. Doxycycline 100 mg PLUS 1-2 g vitamin C can be considered in patients with poorly responsive disease.
Clinical studies
Ongoing clinical trials are evaluating the role of doxycycline in various tumors. In a small pre‑operative breast cancer pilot study (200 mg/day for 2 weeks), doxycycline reduced markers of CSCs (CD44 and ALDH1) in tumor tissue, suggesting it can deplete this resistant subpopulation in patients.(6) Currently evidence of clinical benefit (tumor shrinkage, survival) from doxycycline in solid tumors is lacking. However, doxycycline, was one of the four drugs included in the successful METRICS study. (16)
Types of cancers doxycycline may be beneficial for
Despite the absence of clinical data, doxycycline may have clinical efficacy in the following cancers: melanoma, renal adenocarcinoma, breast cancer, prostate, and malignant gliomas.
Dosing and cautions
The optimal dose and duration of therapy with doxycycline is unknown. The standard dose of doxycycline used in clinical trials is 100 mg twice daily for 12 weeks (ClinTrials.gov). In the METRICS cancer study, doxycycline was given at 100 mg once daily, continuously, alongside the other repurposed metabolic agents for as long as patients remained on the METRICS regimen.
Serious adverse effects are uncommon, with the most common adverse effects being headache and nausea. The effects of doxycycline on the microbiome appear to depend on the dose and duration of therapy. Doxycycline is generally well tolerated clinically, but it is not microbiologically neutral: it can deplete beneficial gut bacteria and select for tetracycline‑resistant strains. Long‑term or repeated courses (months) are more likely to reduce beneficial taxa, lower diversity, and enrich resistant organisms, and these effects can outlast the treatment period. A 100 mg dose is likely to have a lesser detrimental effect on the microbiome. Doxycycline should be rotated monthly with mebendazole (see post on cancer resistance).
If you’ve found this work valuable, please consider upgrading to a paid subscription. Your support helps me continue independent research and share practical, evolving insights—while giving you access to deeper content and more direct engagement.
If you found this article helpful, please restack it to help others discover the Cancer & Metabolic Healing Playbook.
Medical Disclaimer: The discussion of repurposed medications and nutraceuticals in this article is intended to review the scientific literature and does not constitute a recommendation for self-treatment. Decisions regarding the use of off-label therapies should be made in consultation with a qualified healthcare professional familiar with the patient’s medical history and current treatment plan. Please see the full Medical Disclaimer on the introductory page to Marik’s Cancer & Metabolic Healing Playbook.
References
1. Rok J, Rzepka Z, Kowalska J, Banach K, Beberok A, Wrzesniok D. The Anticancer Potential of Doxycycline and Minocycline-A Comparative Study on Amelanotic Melanoma Cell Lines. Int. J Mol. Sci. 2022;23(2).
2. Garrido-Mesa N, Zarzuelo A, Galvez J. Minocycline: far beyond an antibiotic. Br. J Pharmacol. 2013;169(2):337–52.
3. Rok J, Rzepka Z, Beberok A, Pawlik J, Wrzesniok D. Cellular and Molecular Aspects of Anti-Melanoma Effect of Minocycline-A Study of Cytotoxicity and Apoptosis on Human Melanotic Melanoma Cells. Int. J Mol. Sci. 2020;21(18).
4. Rok J, Karkoszka M, Rzepka Z, Respondek M, Banach K, Beberok A, et al. Cytotoxic and proapoptotic effect of doxycycline - An in vitro study on the human skin melanoma cells. Toxicol. In Vitro. 2020;65:104790.
5. Dijk SN, Protasoni M, Elpidorou M, Kroon AM, Taanman JW. Mitochondria as target to inhibit proliferation and induce apoptosis of cancer cells: the effects of doxycycline and gemcitabine. Sci Rep. 2020;10(1):4363.
6. Scatena C, Roncella M, Di Paolo A, Aretini P, Menicagli M, Fanelli G, et al. Doxycycline, an Inhibitor of Mitochondrial Biogenesis, Effectively Reduces Cancer Stem Cells (CSCs) in Early Breast Cancer Patients: A Clinical Pilot Study. Front Oncol. 2018;8:452.
7. De Francesco EM, Bonuccelli G, Maggiolini M, Sotgia F, Lisanti MP. Vitamin C and Doxycycline: A synthetic lethal combination therapy targeting metabolic flexibility in cancer stem cells (CSCs). Oncotarget. 2017;8(40):67269–86.
8. Weiler J, Dittmar T. Minocycline impairs TNF-a induced cell fusion of M13SV1-Cre cells with MDA-MB-435-pFDR1 cells by suppressing NF-kB transcriptional activity and its induction of target-gene expression of fusion-relevant factors. Cell Commun. Signal. 2019;17(1):71.
9. Lokeshwar BL. Chemically modified non-antimicrobial tetracyclines are multifunctional drugs against advanced cancers. Pharmacol. Res. 2011;63(2):146–50.
10. Niu G, Liao Z, Cai L, Wei R, Sun L. The combined effects of celecoxib and minocycline hydrochloride on inhibiting the osseous metastasis of breast cancer in nude mice. Cancer Biother. Radiopharm. 2008;23(4):469–76.
11. Gilbertson-Beadling S, Powers EA, Stamp-Cole M, Scott PS, Wallace TL, Copeland J, et al. The tetracycline analogs minocycline and doxycycline inhibit angiogenesis in vitro by a non-metalloproteinase-dependent mechanism. Cancer Chemother. Pharmacol. 1995;36(5):418–24.
12. Liu FY, Wu YH, Zhou SJ, Deng YL, Zhang ZY, Zhang EL, et al. Minocycline and cisplatin exert synergistic growth suppression on hepatocellular carcinoma by inducing S phase arrest and apoptosis. Oncol. Rep. 2014;32(2):835–44.
13. Masumori N, Tsukamoto T, Miyao N, Kumamoto Y, Saiki I, Yoneda J. Inhibitory effect of minocycline on in vitro invasion and experimental metastasis of mouse renal adenocarcinoma. J Urol. 1994;151(5):1400–4.
14. Markovic DS, Vinnakota K, van RN, Kiwit J, Synowitz M, Glass R, et al. Minocycline reduces glioma expansion and invasion by attenuating microglial MT1-MMP expression. Brain Behav. Immun. 2011;25(4):624–8.
15. Fiorillo M, Tóth F, Sotgia F, Lisanti MP. Doxycycline, Azithromycin and Vitamin C (DAV): A potent combination therapy for targeting mitochondria and eradicating cancer stem cells (CSCs). Aging (Albany NY). 2019;11(8):2202–16.
16. Agrawal S, Vamadevan P, Mazibuko N, Bannister R, Swery R, Wilson S. A new method for ethical and efficient evidence generation for off-label medication use in oncology (A case study in glioblastoma). Front. Pharmacol. 2019;10:681.
All i can say is continue what you are doing and lets hope for the best. Paul
Thank you