

This post MUST be interpreted in conjuction with the next post entitled
“PSA Screening: Promise, Pitfalls, and the Future of Prostate Cancer Detection”
Prostate cancer is one of the most common cancers in men worldwide and a major cause of cancer death, but the individual risk of dying from it is strongly stage‑ and grade‑dependent.(1, 2)
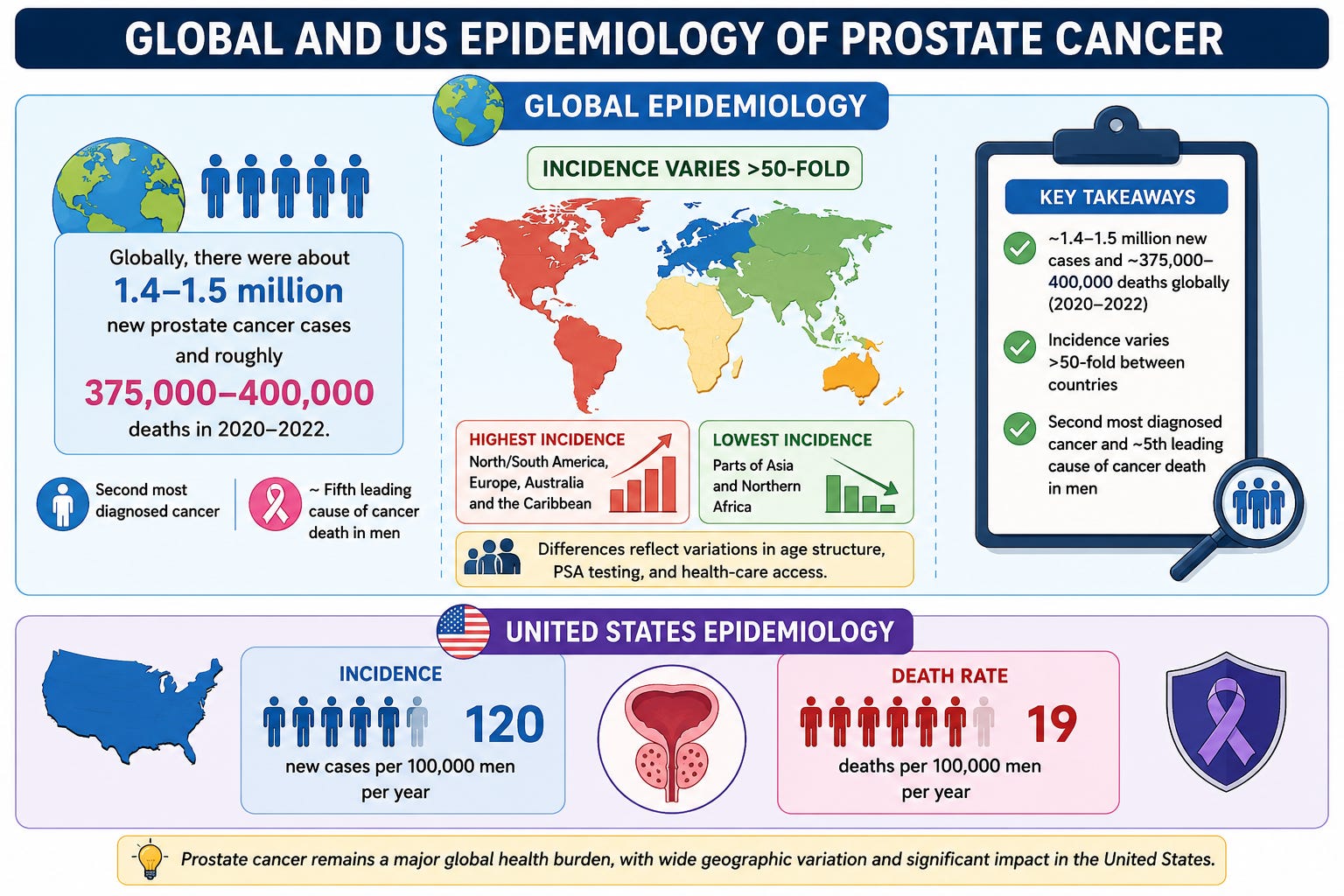
Global and US epidemiology
Globally, there were about 1.4–1.5 million new prostate cancer cases and roughly 375,000–400,000 deaths in 2020–2022, making it the second most diagnosed cancer and about the fifth leading cause of cancer death in men.(1)
Incidence varies more than 50‑fold between countries, highest in North/South America, Europe, Australia and the Caribbean, and lowest in parts of Asia and Northern Africa, reflecting differences in age structure, PSA testing, and health‑care access.(1, 2)
In the United States, the recent incidence rate is about 120 new cases per 100,000 men per year, with a death rate of about 19 per 100,000 men per year.
Lifetime risk and survival
In high‑income settings, a man’s lifetime probability of being diagnosed with prostate cancer is on the order of 12–13%, increasing steeply with age (for example, US data: about 1.8% in men 60–69 vs 9% in men ≥70 years).(3)
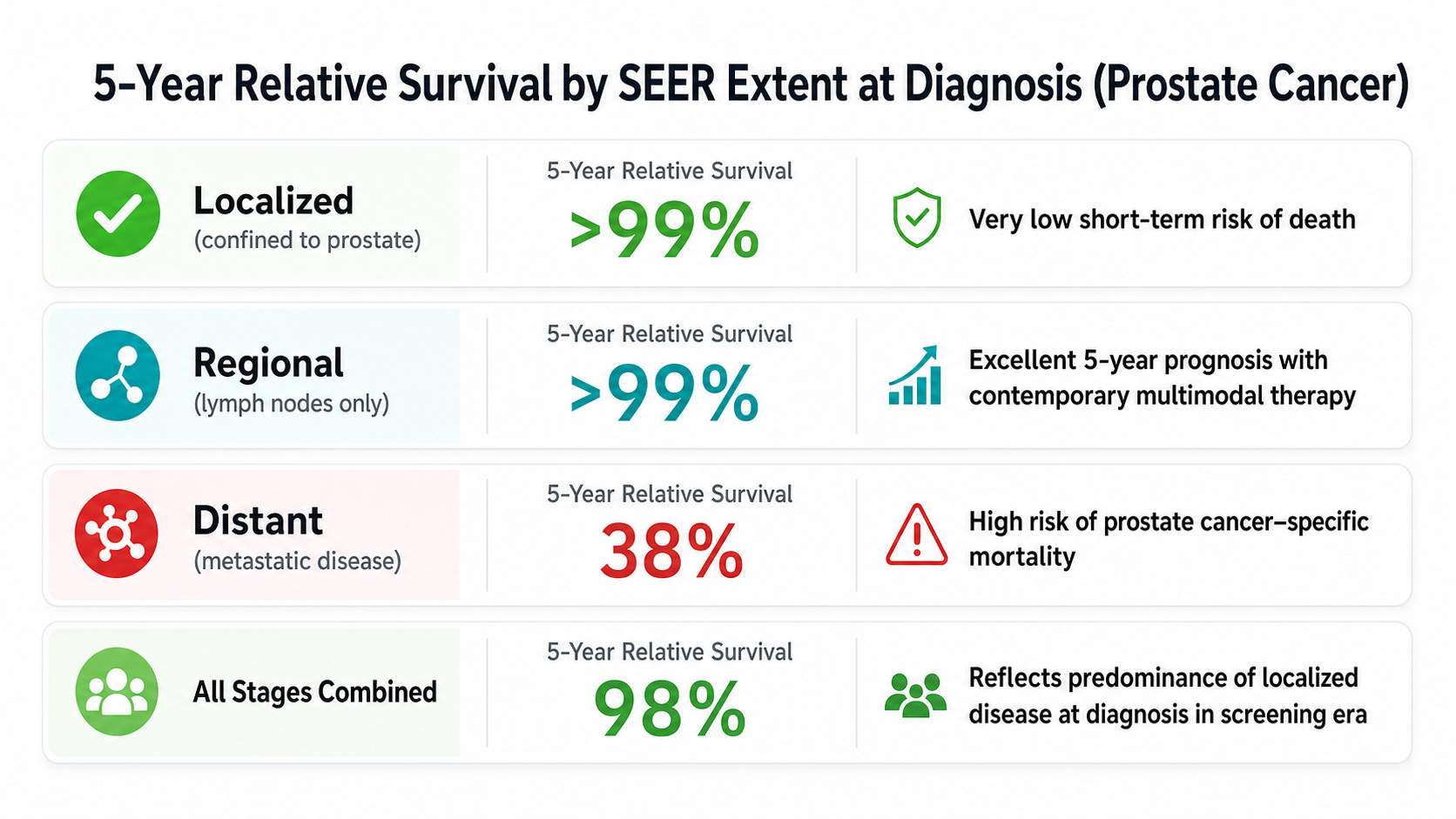
Despite frequent diagnosis, the overall 5‑year relative survival rate in the US is about 97–98%, reflecting the large proportion of localized or regional disease
Who dies of prostate cancer?
Population‑based data from British Columbia show that among men who ultimately died of prostate cancer, about 32% had metastatic, 3% regional (node‑positive), and 39% localized high‑risk disease at presentation; only small fractions had low‑ or intermediate‑risk localized disease.(4)
Median survival from diagnosis to death in that cohort was about 12 years for localized low‑risk, 10 years for localized intermediate‑risk, 6.5 years for localized high‑risk, 4 years for regional, and 1.7 years for metastatic disease at diagnosis.(4)
Key risk factors for developing (and dying from) prostate cancer
Non‑modifiable factors:
Age: Risk rises sharply after age 50; autopsy data show histologic cancer in ~40% of unscreened men >60 and ~60% >80, including a substantial fraction with clinically significant grade groups.(3)
Race/ethnicity: Incidence and mortality are highest in men of African ancestry and lowest in many Asian populations; African‑American men have much higher incidence than men in Africa, underscoring environmental and diagnostic factors.(2)
Family history and genetics: First‑degree relatives with prostate cancer, and germline variants (for example, BRCA2 and other DNA‑repair genes), increase risk and are associated with more aggressive disease and higher prostate‑cancer–specific mortality.(3)
Potentially modifiable factors (evidence strength varies):
Obesity, metabolic syndrome, and physical inactivity are associated with higher risk of advanced or lethal prostate cancer.(2)
Smoking is linked more consistently to prostate cancer mortality than to incidence, suggesting an effect on progression or treatment outcomes.(3)
Table 1. 5 Year survival
How does family history affect prostate cancer risk?
Family history is one of the strongest established risk factors for prostate cancer, and it affects both the chance of developing the disease and, to a lesser extent, the risk of more aggressive or lethal disease.(5)
Magnitude of risk increase
Having a first‑degree relative (father, brother, or son) with prostate cancer roughly doubles to triples a man’s risk of being diagnosed with prostate cancer compared with men without such a history.(6, 7)
Many studies describe a 2–4‑fold increase in risk when a brother or father is affected, with risk generally higher if a brother is affected than if only the father is.(6-9)
If more than one close relative is affected (for example, two or more first‑ or second‑degree relatives), the risk can rise further, with estimates around a 4–5‑fold increase in some series.(8, 9)
Pattern of family history that matters
Risk rises with the number of affected relatives: one first‑degree relative confers a moderate increase; multiple-affected relatives suggest possible hereditary prostate cancer and a substantially higher risk.(8, 9)
Age at diagnosis in the relative is important: if the affected father or brother was diagnosed before about age 60–65, the associated risk for the family member is higher than if the cancer occurred at an older age.(5)
Certain family constellations (for example, three or more first‑degree relatives with prostate cancer, or clustering of prostate plus other related cancers) are used to define hereditary prostate cancer syndromes and warrant genetic evaluation.(5)
Genetics versus shared environment
Twin and family studies estimate that roughly half or more (up to about 60%) of the variation in prostate cancer risk can be attributed to inherited factors, making it one of the most heritable common cancers.(7)
The excess risk in families is driven by a combination of high‑penetrance genes (for example, BRCA2 and other DNA‑repair genes in a minority of families) and many common low‑penetrance variants (polygenic risk), plus shared lifestyle and environmental factors.(5)
Links with breast and other cancers
A family history of breast cancer, especially in close relatives, also modestly increases prostate cancer risk; one large cohort found about a 21% higher overall risk and a roughly similar increase in lethal disease with familial breast cancer alone.(5)
Men with a family history of both prostate and breast cancer had higher risk than those with neither, reflecting shared susceptibility pathways such as BRCA2; this bidirectional association also shows up as higher breast cancer risk in women with male relatives affected by prostate cancer.(5)
Impact on aggressiveness and lethal risk
Family history of prostate cancer is associated not only with higher incidence but also with a higher likelihood of high‑grade or lethal prostate cancer in several cohorts, although estimates vary and screening intensity can confound this.(5)
In one large prospective study, a family history of prostate cancer alone was associated with about a 68% increased risk of total prostate cancer and a roughly 70% increased risk of lethal disease; family history of breast cancer showed a smaller but still elevated risk, especially when both cancers were present in the family.(5)
Table 2. Risk factors for developing prostate cancer
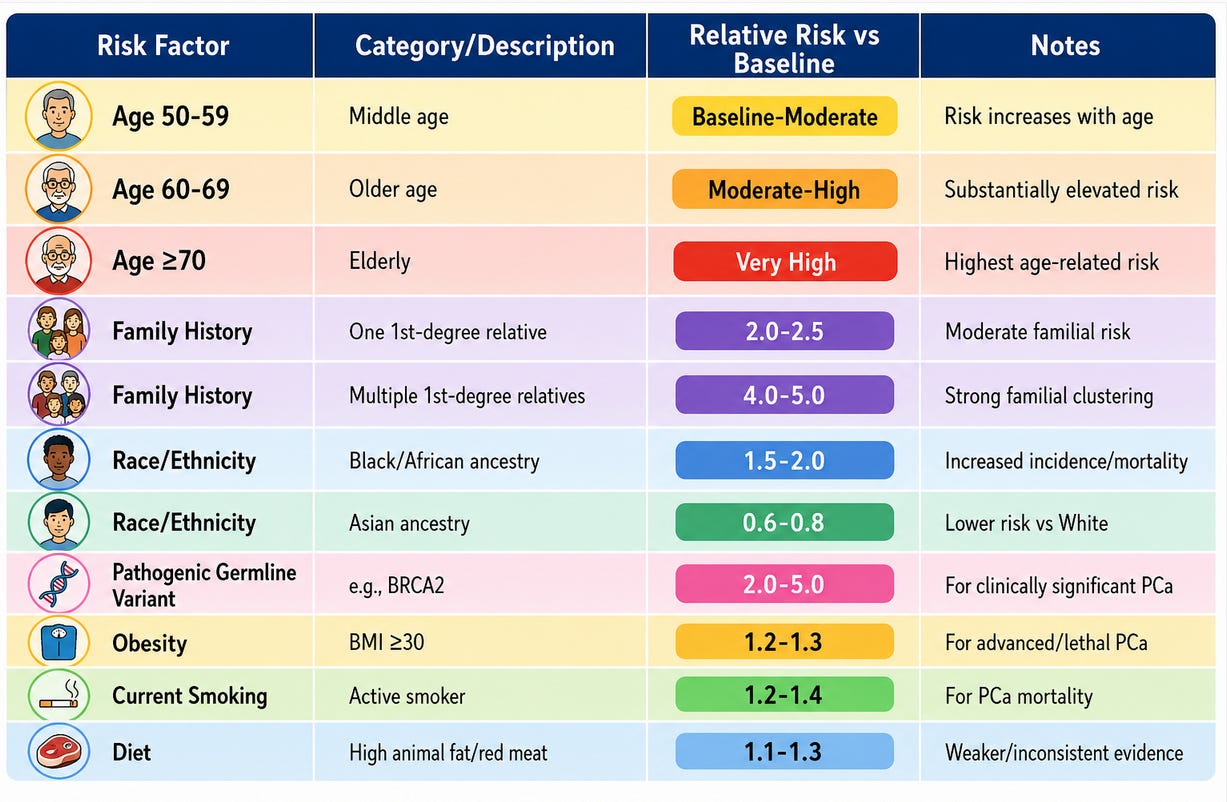
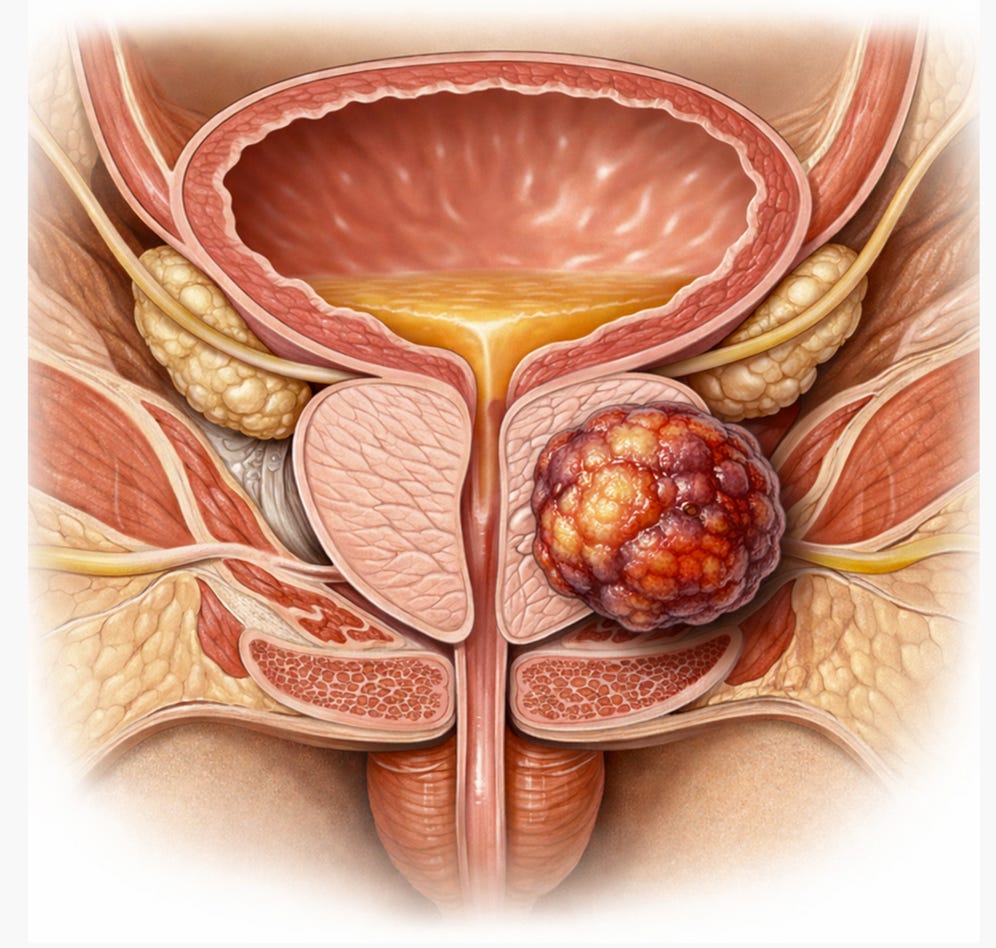
Figure 1. Large prostatic tumor extending beyond the prostate capsule
The Gleason Score
The Gleason score is a grading system that describes how aggressive a prostate cancer looks under the microscope and helps predict behavior and guide treatment.
What the Gleason score is
A pathologist examines prostate biopsy cores and assigns a Gleason grade from 3 to 5 to each cancer pattern, based on how closely the glands resemble normal prostate tissue (3 = more like normal, 5 = very abnormal).
The two most common patterns are added: primary pattern + secondary pattern = Gleason score (for example, 3+4=7 means grade 3 is predominant, grade 4 is the next most common).
In modern practice, reported Gleason scores range from 6 (3+3) to 10 (5+5); 6 is considered low grade, 7 intermediate, and 8–10 high grade.
Table 3. Gleason Score and Risk Prediction
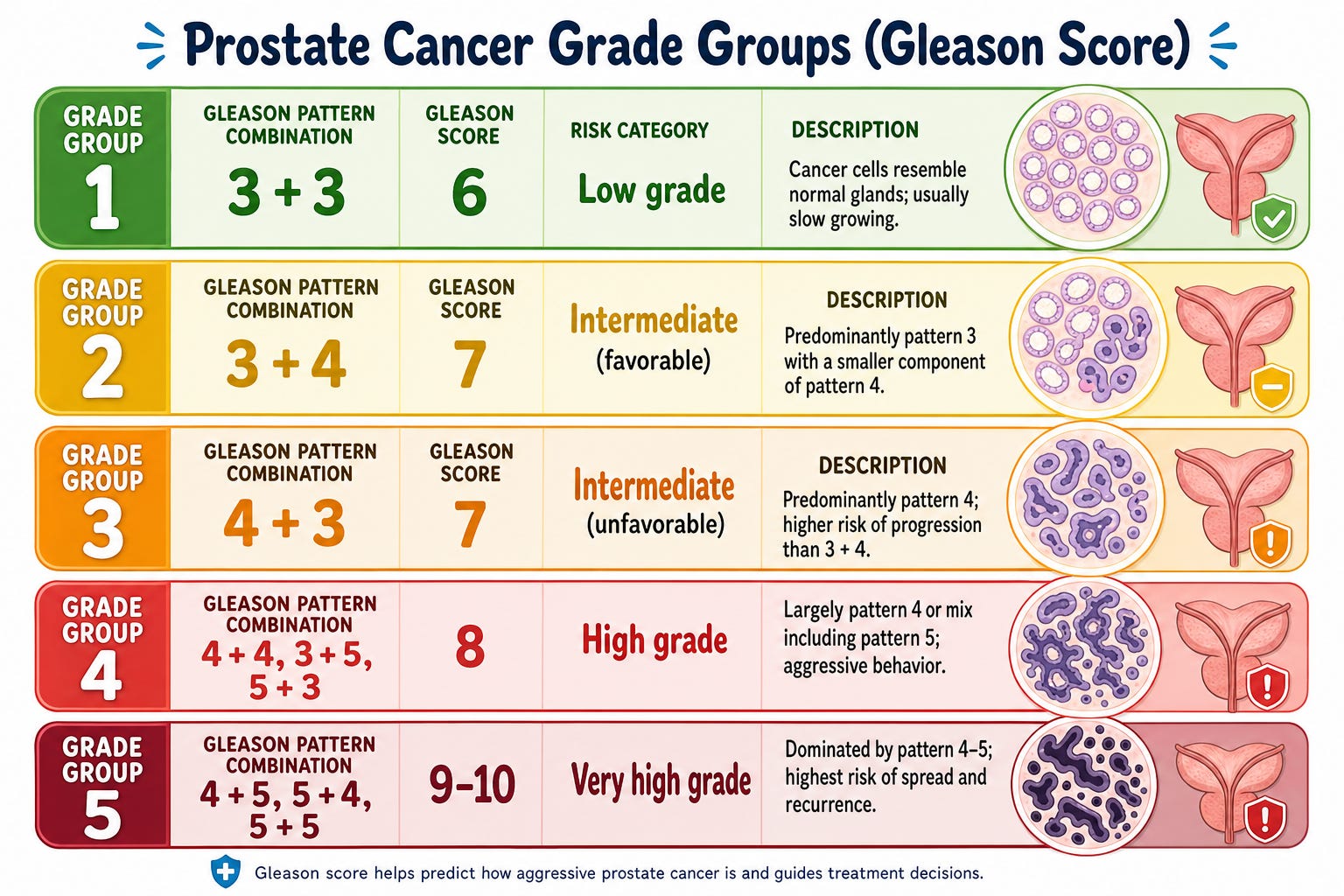
Figure 2. Prostate Cancer Progression
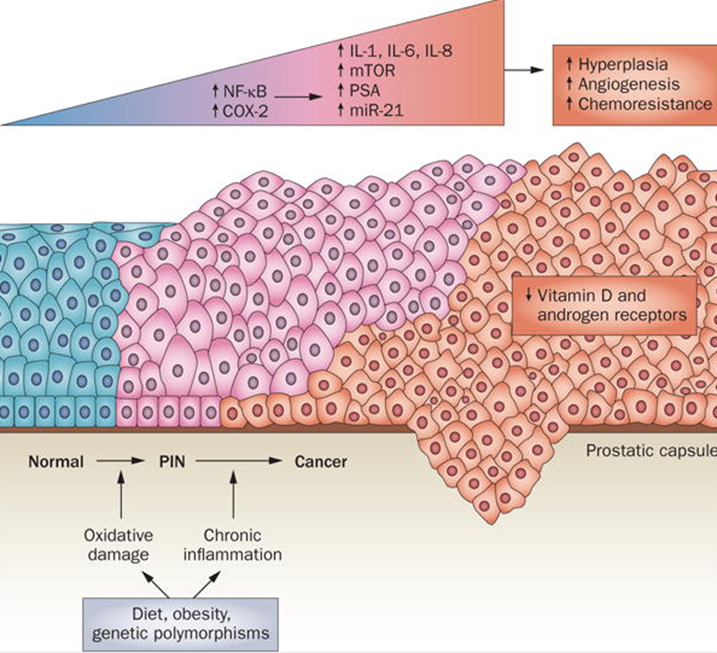
Prostate cancer progression. Accumulated DNA damage, oxidative damage, genetic polymorphisms and chronic inflammation all contribute to disease progression. These events also provide opportunities for possible intervention with chemo preventive agents. Abbreviations: COX-2, cyclooxygenase 2; IL, interleukin; miR, microRNA; mTOR, mammalian target of rapamycin; PIN, prostatic intraepithelial neoplasia; PSA, prostate-specific antigen.
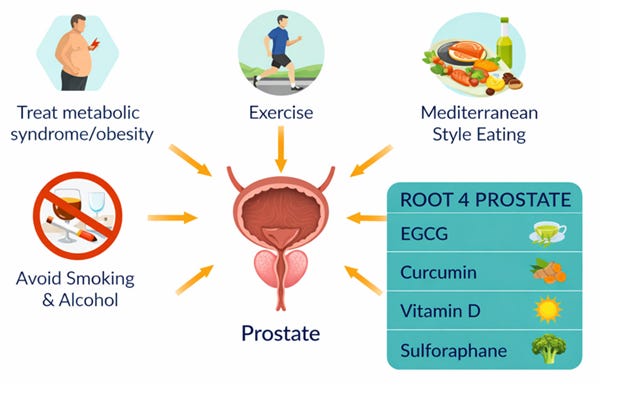
Preventing Prostate Cancer
High‑risk men can substantially lower their chances of developing, or at least of developing aggressive, prostate cancer through a combination of lifestyle, screening, and (in select cases) pharmacologic strategies.(10, 11)
Clarify what “high risk” means
High risk usually refers to one or more of: strong family history, known germline mutation (BRCA2, HOXB13, DNA‑repair genes), African ancestry, or very worrisome PSA history. For such men, prevention and early detection need to be more proactive and individualized than for average‑risk men.(11)
Screening and early detection strategy (see next post)
Start PSA‑based screening earlier than average‑risk men, often around age 40–45, especially with strong family history or known high‑risk mutations and discuss this explicitly with a urologist or oncologist.
Use a risk‑adapted PSA approach:
Very low baseline PSA (for example under about 1–1.5 ng/ml at 45) can justify longer intervals (up to about 5 years in low‑risk men in trials).
Higher baseline PSA (for example ≥1–1.5 ng/ml in the mid‑40s or >3 ng/ml at any age) usually triggers closer follow‑up, MRI, or biopsy depending on the context.
Make screening a shared decision, weighing the benefit of earlier detection against overdiagnosis; U.S. recommendations still emphasize individualized decisions, especially between ages 55–69.
For men with pathogenic germline mutations, follow more intensive, guideline‑based surveillance; some groups recommend annual PSA from 40 or younger, and very low thresholds for MRI/biopsy.(11)
Lifestyle and diet (core measures)
Maintain a healthy weight and avoid central obesity; higher BMI and abdominal fat are linked to more aggressive or lethal prostate cancer.(10, 11)
Exercise regularly: at least 150 minutes/week of moderate‑intensity activity is associated with lower risk of aggressive disease and better metabolic and immune profiles.(10)
Emphasize a Mediterranean‑style eating pattern: high in fish, high in vegetables, fruits, legumes, whole grains, nuts, and olive oil; low in processed meats, refined carbs, and ultra‑processed foods.(10)
Limit high‑fat dairy, excessive calcium, and diets high in saturated fat, which are repeatedly associated with higher prostate cancer risk in observational cohorts.(10)
Intermittent fasting/time restricted eating: intermittent fasting and longer nightly fasting may modestly reduce prostate cancer risk and improve the tumor milieu, but data are limited.
Caloric restriction and intermittent fasting in animal models reduce insulin and IGF‑1, lower glucose availability, induce ketosis, and activate autophagy, all of which can hinder tumor growth and may reduce carcinogenesis.(12)
A Spanish case–control study found that men with a nightly fasting duration >11 hours had a lower odds of prostate cancer than those fasting ≤11 hours (OR 0.77, 95% CI 0.54–1.07),(13)
Earlier work from the same group reported that diurnal eating patterns (early suppers and a longer interval between supper and sleep) were associated with reduced risk of both breast and prostate cancer.(14)
A broader review on time‑restricted eating and cancer concludes that, in theory, aligning eating to circadian rhythms and shortening the eating window may reduce metabolic dysfunction and thereby risk of cancer, but robust prospective human data for specific cancers, including prostate, are not yet available. (15)
Avoid smoking and heavy alcohol; current smoking is linked to higher prostate cancer mortality and overall cancer risk.(10)
Example: A Mediterranean‑style pattern with fish several times weekly, abundant crucifers and tomatoes, nuts, olive oil, and minimal processed meat has been associated with lower prostate cancer incidence in high‑adherence cohorts.(10)
Coffee intake
Higher habitual coffee intake appears modestly associated with a lower risk of overall and especially lethal/high‑grade prostate cancer.
A 2021 BMJ Open systematic review of 15 cohort studies (over 1 million men) found that the highest vs lowest intake category was associated with a relative risk (RR) of 0.91 (95% CI 0.84–0.98) for overall prostate cancer.(16)
In dose–response analysis from this review, risk decreased by about 1% per additional cup per day.(16)
Other meta‑analyses conclude that high coffee intake (≥4–5 cups/day) may be inversely associated with fatal and high‑grade disease.(17)
In the Health Professionals Follow‑up Study, men drinking ≥6 cups/day had a RR of 0.40 (95% CI 0.22–0.75) for lethal prostate cancer vs nondrinkers, with little association for low‑grade or non‑advanced cancers. (18)
The absolute effect size for overall incidence is small (on the order of a 5–10% relative reduction comparing highest vs lowest intake and does not justify recommending large coffee consumption for prostate cancer prevention alone. (19)
Repurposed Drugs and Nutraceuticals to prevent Prostate cancer
EGCG (the main catechin in green tea) shows biological and some clinical signals suggestive of risk reduction for prostate cancer.(20-22)
EGCG and green tea catechins inhibit proliferation, induce apoptosis, modulate androgen receptor, NF‑κB, PI3K/Akt, and epigenetic regulators, and inhibit MMP‑2/9 and angiogenic factors in prostate cancer models.(23)
In TRAMP mouse models, EGCG or green tea polyphenols reduce high‑grade PIN incidence and delay or reduce prostate tumor development. (24)
An In vivo study demonstrates that the combination of polyphenols including EGCG and curcumin has chemo-preventative properties.(25)
Several observational studies and pooled analyses report that higher green tea intake is associated with lower prostate cancer incidence or mortality, particularly in East Asian populations with high consumption.(26)
In short pre‑prostatectomy studies (6–8 weeks of Polyphenol E, 500–800 mg EGCG/day) show EGCG is detectable in plasma and sometimes in prostate tissue, and can lower PSA, HGF, VEGF, and oxidative DNA damage markers without major toxicity.(27)
An early Italian RCT in men with high‑grade PIN using green tea catechins (including about 600 mg/day EGCG) for one year reported 1/30 cancers in the catechin arm vs 9/30 in placebo, suggesting a large relative risk reduction in progression, with good tolerability (High-grade prostatic intraepithelial neoplasia - HGPIN or high-grade PIN- is a precancerous condition where prostate cells appear abnormal under a microscope but have not yet spread outside the gland).
A pooled analysis of trials in men with HGPIN or Atypical Small Acinar proliferation (ASAP) found 7.9% prostate cancer in the catechin arm vs 22% in placebo, with a pooled risk ratio of 0.41 (95% CI 0.19–0.86), suggesting a statistically significant reduction in progression in this specific high‑risk group.(28)
Standardized, decaffeinated green tea catechin preparations containing 400–800 mg EGCG/day for months to a year are generally well tolerated, with RCTs reporting no significant increase in hepatotoxicity versus placebo when monitored.(22)
Rare cases of EGCG‑related hepatotoxicity have been reported with some high‑dose supplements; many trials include liver enzyme monitoring, and using standardized preparations and taking them with food is typical risk‑mitigation.(22)
Curcumin: Curcumin has plausible biologic activity and encouraging preclinical and clinical data for prostate cancer chemoprevention, but definitive evidence that it prevents prostate cancer in humans is still lacking.
Curcumin inhibits multiple pathways implicated in prostate carcinogenesis, including PI3K/Akt/mTOR, NF‑κB, and androgen receptor (AR) signaling, leading to anti‑proliferative, pro‑apoptotic, anti‑angiogenic, and anti‑metastatic effects in cell and animal models.(29)
A meta‑analysis of eight clinical studies (638 participants) reported that curcumin significantly reduced prostate cancer incidence/tumor occurrence with a pooled effect size of −0.91 (95% CI −1.68 to −0.14).(30)
In men with prior negative biopsies but elevated PSA, a supplement combining soy and curcumin was associated with marked PSA reductions in those with PSA >10 ng/mL, supporting a potential effect on prostate biology but not proving primary cancer prevention.(31)
A randomized, double‑blind, placebo‑controlled trial in men on intermittent androgen deprivation found that adding oral curcumin for 6 months significantly reduced PSA progression during the treatment period (10.3% vs 30.2%, P ≈ 0.026), without added toxicity, suggesting disease‑modifying activity in established prostate cancer rather than primary prevention.(32)
A recent systematic review of preclinical prostate cancer models concludes that curcumin has robust multi‑targeted anticancer activity and that nanoparticle formulations (e.g., Theracurmin) can suppress PI3K/Akt signaling in early‑stage disease in a pattern consistent with chemoprevention.(29)
Vitamin D: The role of Vitamin D in the prevention of prostate cancer is controversial. Overall, vitamin D supplementation has been associated with a reduced risk of cancer. (33, 34) Vitamin D deficiency is associated with a higher risk of prostate cancer. However, several studies have reported a “U” shaped or “J” shaped association between vitamin D levels and risk of prostate cancer; it is likely that this is a statistical artifact (see below).
Several observational studies and pooled analyses suggest that vitamin D deficiency is linked to a higher risk of prostate cancer, especially more aggressive disease and in populations with limited sun exposure.(35)
Vitamin D deficiency has been demonstrated to increase the risk of breast cancer while supplemental vitamin D intake had an inverse relationship with this outcome. (36) Both prospective and retrospective epidemiologic studies indicate that levels of 25-hydroxyvitamin D below 20 ng per milliliter are associated with a 30 to 50% increased risk of incident colon, prostate, and breast cancer, along with higher mortality from these cancers. (37)
However, a large, pooled analysis of 19 prospective studies (12,824 cases, 35,583 participants) found that higher circulating 25‑OH vitamin D was associated with a modestly increased prostate cancer risk (RR 1.15 for highest vs lowest category; ~4% increase in risk per 10 ng/mL increase).(38)
Furthermore, several large cohorts and nested case‑control studies have reported that men with higher 25‑OH D levels are at increased risk of being diagnosed with prostate cancer, including higher‑grade disease in some analyses.(39)
At least one large prospective analysis has reported a U-shaped curve: both low and high 25(OH)D concentrations were associated with increased prostate cancer risk, particularly for high‑grade disease.(40)
In patients with cancer we target a Vitamin D3 level, close to 100 ng/l. This is a controversial topic, and it is unclear whether a level of between 100-150 ng/ml is harmful if serum calcium and PTH levels are monitored (Coimbra protocol).(41-43) It is likely that the target level differs for maintaining good health and preventing cancer. There is no single universally accepted “target” 25(OH)D level for cancer prevention, but most of the stronger epidemiologic and interventional data point to benefit once levels are at least around 30–40 ng/mL, with many groups aiming for a level of 40 -60 ng/mL as a pragmatic threshold.(44, 45)
It is likely that the J and U-shaped association between vitamin D levels and risk of prostate cancer is a statistical anomaly (personal communication with Dr Sunil Wimalawansa). This association has not been convincingly proven nor replicated in studies with adequate statistical power. This issue has been examined by Dr Wimalawansa and others.(46, 47) He found that beyond approximately 60 ng/mL (especially beyond 80 ng/mL), the number of subjects becomes minuscule. The data scatter is substantial, rendering interpretations and extrapolations at higher serum 25(OH)D levels statistically unreliable. For example, when comparing the number of subjects below 30 ng/mL with those above 60 ng/mL, the latter group constitutes less than 8% of the total sample; above 80 ng/mL, it is less than 3%. It is scientifically “unsound” and incorrect to extrapolate from such sparse and highly scattered data at the upper end of the curve, particularly given the potential for inherent and observer biases.
Figure 3. Optimal Vitamin D level

Sulforaphane: Sulforaphane appears to be a promising multi‑target chemopreventive agent for prostate carcinogenesis, with robust mechanistic and preclinical support but only modest, early-phase human data so far.(48)
Androgen receptor (AR) signaling: Sulforaphane reduces AR expression by interacting with the AR gene promoter and destabilizing the AR protein (via HDAC6 inactivation), thereby suppressing AR-driven growth.(49)
Direct effects on tumor biology: In prostate cancer cell lines (LNCaP, PC‑3, others), sulforaphane decreases proliferation, migration, and invasion and promotes apoptosis in a dose‑dependent fashion, including via microRNA‑mediated pathways (e.g., miR‑3919).(50)
Inflammation and oxidative stress: By activating Nrf2 and modulating related pathways, sulforaphane reduces oxidative damage and inflammatory signaling that contributes to prostate carcinogenesis.(48)
Higher intake of cruciferous vegetables (broccoli, cauliflower, etc.), a major dietary source of sulforaphane, is associated with lower overall and prostate cancer risk in observational studies.(51)
Review articles focused on prostate cancer conclude that sulforaphane-rich diets reduce incidence and severity of prostate tumors in the TRAMP mouse model, supporting a chemo-preventive role. (52)
Biochemical recurrence trial: In a phase II single‑arm study of 20 men with PSA recurrence after prostate cancer treatment, 200 μmol/day sulforaphane‑rich broccoli sprout extract for up to 20 weeks significantly lengthened PSA doubling time from 6.1 to 9.6 months (p = 0.044), with good tolerability.(53)
Current evidence supports sulforaphane as a biologically plausible chemopreventive agent for prostate cancer, acting through AR suppression, Nrf2 activation, HDAC inhibition, and broader epigenetic and anti‑inflammatory effects. (48)
Metformin and statins have been suggested lower prostate cancer incidence or mortality, particularly for aggressive disease, however the data is conflicting. (54)
A 2024 meta‑analysis of observational studies found that metformin use was associated with reduced prostate cancer incidence (RR ≈ 0.82, 95% CI 0.74–0.91), with a stronger effect with longer duration of use.(55)
Other large studies and nested analyses have reported no reduction or even neutral/positive associations, especially when better adjustment for PSA testing patterns, glycemic control, and obesity is included.(56, 57)
Importantly, one well‑controlled trial in men on active surveillance (MAST) reported that metformin did not slow progression of low‑risk disease, underscoring that benefit is not universal across disease states.(58)
Overall, the epidemiologic data point to a possible risk reduction mainly in men with type 2 diabetes already taking metformin but confounding and heterogeneity mean causality is uncertain.(56)
Statins do not appear to meaningfully reduce overall prostate cancer incidence at usual doses, but they are consistently associated with lower risk of advanced/fatal disease and better prognosis once prostate cancer is present.(59, 60)
Large meta-analyses of RCTs and cohort studies show no significant reduction in overall incident prostate cancer with statin use (pooled RR around 0.94, 95% CI 0.82–1.08).(59)
A meta-analysis cited in a recent review found statin use associated with about 20% lower risk of advanced prostate cancer (RR 0.80, 95% CI 0.70–0.90). (60)
A 2022 systematic review and meta-analysis found statin use associated with reduced prostate cancer–specific mortality (pooled HR 0.76, 95% CI 0.69–0.84).(61)
Current evidence does not support prescribing statins solely to prevent prostate cancer in average‑risk men, as overall incidence reduction is small or null and data are largely observational.
Omega-3-Fatty acids: Omega-3 fatty acids may modestly reduce prostate cancer risk and slow progression at dietary (food-based) intakes, but the data are mixed and high-dose supplementation has not been proven preventive and may even associate with higher mortality or risk at very high blood levels.(62)
Several prospective cohorts (PLCO, AARP, Augustsson et al.) link higher dietary marine omega-3 intake (fish-based EPA/DHA) with a lower incidence of prostate cancer or aggressive disease, although effect sizes are small and often attenuate after multivariable adjustment.(62)
In contrast, SELECT secondary analyses associated higher plasma long‑chain omega‑3s with higher prostate cancer incidence and higher risk of high‑grade disease, but this was observational, not a supplement trial, and cannot establish causality.(63)
Observational work suggests higher fish/omega‑3 intake is associated with better survival among men with existing prostate cancer and lower risk of aggressive phenotypes. (62)
Current evidence does not support high‑dose omega‑3 supplementation as a primary prostate cancer prevention strategy. A reasonable, evidence‑aligned approach is: emphasize regular consumption of fatty fish (e.g., 1–2 servings/week) providing modest marine omega‑3 intakes; avoid extreme or supraphysiologic doses of omega‑3 supplements solely for prostate cancer prevention; and focus on broader dietary patterns and established prevention measures (weight control, physical activity, smoking avoidance).
Aged garlic extract: Aged garlic/black garlic extracts show anti-inflammatory and antiproliferative effects in prostate models and epidemiology suggests garlic consumption may modestly reduce prostate cancer risk but there is no direct clinical trial evidence that aged garlic extract prevents prostate cancer in humans yet. (64)
Resveratrol: A clinical review notes that despite promising in vitro and animal data, there is no proof from human clinical trials that resveratrol prevents or treats prostate diseases, and no clear evidence from intervention trials in men at risk.(65)
Berberine: Berberine has multiple prostate-relevant anticancer mechanisms in vitro and in animals, but there are essentially no human data showing that it prevents prostate cancer.(66) Hence, berberine is best viewed as a promising preclinical agent with mechanisms compatible with chemoprevention.
Lycopene: Lycopene intake from foods like tomatoes is plausibly protective, but current human evidence is insufficient to recommend lycopene supplements as a stand‑alone preventive.
A 2011 systematic review of randomized trials (Cochrane Review) concluded that there is insufficient evidence to support or refute lycopene supplementation for prostate cancer prevention. (67)
Randomized trials of lycopene supplements in men at elevated prostate risk (e.g., high‑grade PIN or prior negative biopsies) have not shown clear, consistent reductions in PSA or progression risk.(68)
Any use of these agents for “prevention” should be individualized, considering metabolic status and patient preference.
Figure 4. Preventing Prostate Cancer
If you’ve found this work valuable, please consider upgrading to a paid subscription. Your support helps me continue independent research and share practical, evolving insights—while giving you access to deeper content and more direct engagement.
New Here?
Start with the: Cancer and the Metabolic Library

Medical Disclaimer: The discussion of repurposed medications and nutraceuticals in this article is intended to review the scientific literature and does not constitute a recommendation for self-treatment. Decisions regarding the use of off-label therapies should be made in consultation with a qualified healthcare professional familiar with the patient’s medical history and current treatment plan. Please see the full Medical Disclaimer on the introductory page to Marik’s Cancer & Metabolic Healing Playbook.
References
1. Wang L, Lu B, He M, Wang Y, Wang Z, Du L. Prostate Cancer Incidence and Mortality: Global Status and Temporal Trends in 89 Countries From 2000 to 2019. Front Public Health. 2022;10:811044.
2. Rawla P. Epidemiology of Prostate Cancer. World Journal of Oncology. 2019;10:63–89.
3. Bergengren O, Pekala KR, Matsoukas K, Fainberg J, Mungovan SF, Bratt O, et al. 2022 Update on Prostate Cancer Epidemiology and Risk Factors-A Systematic Review. Eur Urol. 2023;84(2):191–206.
4. Parimi S, Bondy S, Aparicio M, Sunderland K, Cho J, Bachand F, et al. Presenting stage and risk group in men dying of prostate cancer. Curr Oncol. 2020;27(6):e547–e51.
5. Barber LM, Gerke T, Markt SC, Peisch SF, Wilson KM, Ahern T, et al. Family history of breast or prostate cancer and prostate cancer risk. Clin. Cancer Res. 2018;24:5910–7.
6. Clements MB, Vertosick EA, Guerrios-Rivera L, De Hoedt AM, Hernandez J, Liss MA, et al. Defining the Impact of Family History on Detection of High-grade Prostate Cancer in a Large Multi-institutional Cohort. Eur Urol. 2022;82(2):163–9.
7. Mucci LA, Hjelmborg JB, Harris JR, Czene K, Havelick DJ, Scheike T, et al. Familial Risk and Heritability of Cancer Among Twins in Nordic Countries. Jama. 2016;315(1):68–76.
8. Seibert TM, Garraway IP, Plym A, Mahal BA, Giri V, Jacobs MF, et al. Genetic Risk Prediction for Prostate Cancer: Implications for Early Detection and Prevention. Eur Urol. 2023;83(3):241–8.
9. Huynh-Le MP, Karunamuni R, Fan CC, Asona L, Thompson WK, Martinez ME, et al. Prostate cancer risk stratification improvement across multiple ancestries with new polygenic hazard score. Prostate Cancer Prostatic Dis. 2022;25(4):755–61.
10. Obeagu EI. Prostate cancer risk reduction: promising prevention practices and insights. Ann Med Surg (Lond). 2025;87(7):4344–55.
11. Plym A, Zhang Y, Stopsack KH, Delcoigne B, Wiklund F, Haiman C, et al. A Healthy Lifestyle in Men at Increased Genetic Risk for Prostate Cancer. Eur Urol. 2023;83(4):343–51.
12. Kalam F, James DL, Li YR, Coleman MF, Kiesel VA, Cespedes Feliciano EM, et al. Intermittent fasting interventions to leverage metabolic and circadian mechanisms for cancer treatment and supportive care outcomes. J Natl Cancer Inst Monogr. 2023;2023(61):84–103.
13. Palomar-Cros A, Espinosa A, Straif K, Pérez-Gómez B, Papantoniou K, Gómez-Acebo I, et al. The Association of Nighttime Fasting Duration and Prostate Cancer Risk: Results from the Multicase-Control (MCC) Study in Spain. Nutrients. 2021;13(8).
14. Kogevinas M, Espinosa A, Castelló A, Gómez-Acebo I, Guevara M, Martin V, et al. Effect of mistimed eating patterns on breast and prostate cancer risk (MCC-Spain Study). Int J Cancer. 2018;143(10):2380–9.
15. Shams-White MM, Goldbaum AA, Agurs-Collins T, Czajkowski S, Herrick KA, Nebeling L, et al. Time-restricted eating and cancer: lessons learned and considerations for a path forward. J Natl Cancer Inst. 2025;117(7):1311–5.
16. Chen X, Zhao Y, Tao Z, Wang K. Coffee consumption and risk of prostate cancer: a systematic review and meta-analysis. BMJ Open. 2021;11(2):e038902.
17. Lu Y, Zhai L, Zeng J, Peng Q, Wang J, Deng Y, et al. Coffee consumption and prostate cancer risk: an updated meta-analysis. Cancer Causes Control. 2014;25(5):591–604.
18. Wilson KM, Kasperzyk JL, Rider JR, Kenfield S, van Dam RM, Stampfer MJ, et al. Coffee consumption and prostate cancer risk and progression in the Health Professionals Follow-up Study. J Natl Cancer Inst. 2011;103(11):876–84.
19. Xia J, Chen J, Xue JX, Yang J, Wang ZJ. An Up-to-date Meta-analysis of Coffee Consumption and Risk of Prostate Cancer. Urol J. 2017;14(5):4079–88.
20. Gupta S, Ahmad N, Nieminen AL, Mukhtar H. Growth inhibition, cell-cycle dysregulation, and induction of apoptosis by green tea constituent (-)-epigallocatechin-3-gallate in androgen-sensitive and androgen-insensitive human prostate carcinoma cells. Toxicol. Appl. Pharmacol. 2000;164(1):82–90.
21. Rogovskii VS, Popov SV, Sturov NV, Shimanovskii NL. The Possibility of Preventive and Therapeutic Use of Green Tea Catechins in Prostate Cancer. Anticancer Agents Med Chem. 2019;19(10):1223–31.
22. Kumar NB, Dickinson SI, Schell MJ, Manley BJ, Poch MA, Pow-Sang J. Green tea extract for prevention of prostate cancer progression in patients on active surveillance. Oncotarget. 2018;9(102):37798–806.
23. Naponelli V, Ramazzina I, Lenzi C, Bettuzzi S, Rizzi F. Green Tea Catechins for Prostate Cancer Prevention: Present Achievements and Future Challenges. Antioxidants (Basel). 2017;6(2).
24. Fujiki H, Watanabe T, Sueoka E, Rawangkan A, Suganuma M. Cancer Prevention with Green Tea and Its Principal Constituent, EGCG: from Early Investigations to Current Focus on Human Cancer Stem Cells. Mol Cells. 2018;41(2):73–82.
25. Wang P, Wang B, Chung S, Wu Y, Henning SM, Vadgama JV. Increased chemopreventive effect by combining arctigenin, green tea polyphenol and curcumin in prostate and breast cancer cells. RSC Adv. 2014;4(66):35242–50.
26. Bailey HH, Mukhtar H. Green Tea Polyphenols and Cancer Chemoprevention of Genitourinary Cancer. Am Soc Clin Oncol Educ Book 2013; 33:92–6.
27. Kumar M, Verma S, Rawat S, Dhatwalia SK. Exploring integrative approaches: EGCG’s potential in combating prostate cancer. World Cancer Research Journal 2024;11:e2744.
28. Perletti G, Magri V, Vral A, Stamatiou K, Trinchieri A. Green tea catechins for chemoprevention of prostate cancer in patients with histologically-proven HG-PIN or ASAP. Concise review and meta-analysis. Arch Ital Urol Androl. 2019;91(3).
29. Esmaeli M, Dehghanpour Dehabadi M. Curcumin in prostate cancer: a systematic review of molecular mechanisms and nanoformulated therapeutic strategies. BMC Cancer. 2025;25(1):1609.
30. Shirdel A, Zargaran FZ, Meshkat M, Amirabadi A. Clinical Antitumor effects of Curcumin in Prostate Cancer Environment: A Meta-Analysis. Novelty in Biomedicine. 2025;4:233–9.
31. Thompson IM, Jr., Cabang AB, Wargovich MJ. Future directions in the prevention of prostate cancer. Nat Rev Clin Oncol. 2014;11(1):49–60.
32. Choi YH, Han DH, Kim SW, Kim MJ, Sung HH, Jeon HG, et al. A randomized, double-blind, placebo-controlled trial to evaluate the role of curcumin in prostate cancer patients with intermittent androgen deprivation. Prostate. 2019;79(6):614–21.
33. Bischoff-Ferrari HA, Vellas B, Rizzoli R, Kressig RW. Effect of Vitamin D supplementation, omega-3 fatty acid supplementation, or a strengh-training excercise program on clinical outcomes in older adults. the DO-HEALTH randomized clinical trial. JAMA. 2020;324:1855–68.
34. Bischoff-Ferrari HA, Willett WC, Manson JE, Dawson-Hughes B, Manz MG, Theller R, et al. Combined Vitamin D, omega-3 fatty acids, and a simple home exercise program may reduce cancer risk among active adults aged 70 and older: A randomized clinical trial. Front. Aging. 2022;3:852643.
35. Cassell A, Konneh S. Unlocking the potential-vitamin D in prostate cancer prevention. World J Clin Oncol. 2024;15(2):169–74.
36. Hossain S, Beydoun MA, Beydoun HA, Chen X, Zonderman AB, Wood RJ. Vitamin D and breast cancer: A systematic review and meta-analysis of observational studies. Clin. Nutr. ESPEN. 2019;30:170–84.
37. Holick MF. Vitamin D deficiency. N. Engl. J. Med. 2002;357:266–81.
38. Gao J, Wei W, Wang G, Zhou H, Fu Y, Liu N. Circulating vitamin D concentration and risk of prostate cancer: a dose-response meta-analysis of prospective studies. Ther Clin Risk Manag. 2018;14:95–104.
39. Albanes D, Mondul AM, Yu K, Parisi D, Horst RL, Virtamo J, et al. Serum 25-hydroxy vitamin D and prostate cancer risk in a large nested case-control study. Cancer Epidemiol Biomarkers Prev. 2011;20(9):1850–60.
40. Kristal AR, Till C, Song X, Tangen CM, Goodman PJ, Neuhauser ML, et al. Plasma vitamin D and prostate cancer risk: results from the Selenium and Vitamin E Cancer Prevention Trial. Cancer Epidemiol Biomarkers Prev. 2014;23(8):1494–504.
41. Finamor DC, Sinigaglia-Coimbra R, Neves LC, Gutierrez M, Silva JJ, Torres LD, et al. A pilot study assessing the effect of prolonged administration of high daily doses of vitamin D on the clinical course of vitiligo and psoriasis. Dermatoendocrinol. 2013;5(1):222–34.
42. Amon U, Yaguboglu R, Ennis M, Holick MF, Amon J. Safety Data in Patients with Autoimmune Diseases during Treatment with High Doses of Vitamin D3 According to the “Coimbra Protocol”. Nutrients. 2022;14(8).
43. Lemke D, Klement RJ, Schweiger F, Schweiger B, Spitz J. Vitamin D resistance as a possible cause of autoimmune diseases: A hypothesis confirmed by a therapeutic high-dose Vitamin D protocol. Front. Immunol. 2021;12:655739.
44. Bischoff-Ferrari HA. Optimal serum 25-hydroxyvitamin D levels for multiple health outcomes. Adv Exp Med Biol. 2014;810:500–25.
45. Ekmekcioglu C, Poteser M. The Optimal Protective 25-Hydroxyvitamin D Level for Different Health Outcomes in Adults: A Brief Summary of Dose-Response Meta-Analyses. Metabolites. 2025;15(4).
46. Kojima G, Iliffe S, Tanabe M. Vitamin D supplementation as a potential cause of U-shaped associations between vitamin D levels and negative health outcomes: a decision tree analysis for risk of frailty. BMC Geriatr. 2017;17(1):236.
47. Grant WB, Wimalawansa SJ, Pludowski P, Cheng RZ. Vitamin D: Evidence-Based Health Benefits and Recommendations for Population Guidelines. Nutrients. 2025;17(2).
48. Mordecai J, Ullah S, Ahmad I. Sulforaphane and Its Protective Role in Prostate Cancer: A Mechanistic Approach. Int J Mol Sci. 2023;24(8).
49. Gibbs A, Schwartzman J, Deng V, Alumkal J. Sulforaphane destabilizes the androgen receptor in prostate cancer cells by inactivating histone deacetylase 6. Proc Natl Acad Sci U S A. 2009;106(39):16663–8.
50. Zhang F, Wan X, Zhan J, Shen M, Li R. Sulforaphane inhibits the growth of prostate cancer by regulating the microRNA-3919/DJ-1 axis. Front Oncol. 2024;14:1361152.
51. Clarke JD, Dashwood RH, Ho E. Multi-targeted prevention of cancer by sulforaphane. Cancer Lett. 2008;269(2):291–304.
52. Amjad AI, Parikh RA, Appleman LJ, Hahm ER, Singh K, Singh SV. Broccoli-Derived Sulforaphane and Chemoprevention of Prostate Cancer: From Bench to Bedside. Curr Pharmacol Rep. 2015;1(6):382–90.
53. Alumkal JJ, Slottke R, Schwartzman J, Cherala G, Munar M, Graff JN, et al. A phase II study of sulforaphane-rich broccoli sprout extracts in men with recurrent prostate cancer. Invest New Drugs. 2015;33(2):480–9.
54. Koo HY, Jeong SM, Cho MH, Chun S, Shin DW, Park J. Population-wide impacts of aspirin, statins, and metformin use on prostate cancer incidence and mortality. Sci Rep. 2021;11(1):16171.
55. Liu Y, Zhang Q, Huang X. Effect of metformin on incidence, recurrence, and mortality in prostate cancer patients: integrating evidence from real-world studies. Prostate Cancer Prostatic Dis. 2025;28(1):210–9.
56. Feng T, Sun X, Howard LE, Vidal AC, Gaines AR, Moreira DM, et al. Metformin use and risk of prostate cancer: results from the REDUCE study. Cancer Prev Res (Phila). 2015;8(11):1055–60.
57. Freedman LS, Agay N, Farmer R, Murad H, Olmer L, Dankner R. Metformin Treatment Among Men With Diabetes and the Risk of Prostate Cancer: A Population-Based Historical Cohort Study. Am J Epidemiol. 2022;191(4):626–35.
58. Fleshner NE, Bernardino RM, Izawa J, Drachenberg D, Saranchuk JW, Fairey A, et al. Metformin Active Surveillance Trial in Low-Risk Prostate Cancer. J Clin Oncol. 2025;43(34):3662–71.
59. Xu MY, An Y, Liu CQ, Xu JZ, Zhong XY, Zeng N, et al. Association of Statin Use with the Risk of Incident Prostate Cancer: A Meta-Analysis and Systematic Review. J Oncol. 2022;2022:7827821.
60. Craig EL, Stopsack KH, Evergren E, Penn LZ, Freedland SJ, Hamilton RJ, et al. Statins and prostate cancer-hype or hope? The epidemiological perspective. Prostate Cancer Prostatic Dis. 2022;25(4):641–9.
61. An Y, Sun JX, Xu MY, Liu CQ, Xu JZ, Zhong XY, et al. Statin Use Is Associated with Better Prognosis of Patients with Prostate Cancer after Definite Therapies: A Systematic Review and Meta-Analysis of Cohort Studies. J Oncol. 2022;2022:9275466.
62. Shu X, Lin J, Yao L, Liu S, Chen Q, Wang H, et al. Dietary Omega-3 intake may slow prostate cancer progression and reduce mortality risk: evidence from prostate, lung, colorectal, and ovarian cancer screening trial. Front Nutr. 2025;12:1623295.
63. Alexander W. Prostate cancer risk and omega-3 Fatty Acid intake from fish oil: a closer look at media messages versus research findings. P t. 2013;38(9):561–4.
64. Miraghajani M, Rafie N, Hajianfar H, Larijani B, Azadbakht L. Aged Garlic and Cancer: A Systematic Review. Int J Prev Med. 2018;9:84.
65. Jasiński M, Jasińska L, Ogrodowczyk M. Resveratrol in prostate diseases - a short review. Cent European J Urol. 2013;66(2):144–9.
66. Lu W, Du S, Wang J. Berberine inhibits the proliferation of prostate cancer cells and induces G₀/G₁ or G₂/M phase arrest at different concentrations. Mol Med Rep. 2015;11(5):3920–4.
67. Ilic D, Forbes KM, Hassed C. Lycopene for the prevention of prostate cancer. Cochrane Database Syst Rev. 2011;2011(11):Cd008007.
68. Kumar NB, Besterman-Dahan K, Kang L, Pow-Sang J, Xu P, Allen K, et al. Results of a Randomized Clinical Trial of the Action of Several Doses of Lycopene in Localized Prostate Cancer: Administration Prior to Radical Prostatectomy. Clin Med Urol. 2008;1:1–14.
Thanks...
Continue what you are doing and see how he tolerates the oncology treatment. He does not need to complete if he tolerates poorly.