
Why Randomized Controlled Trials Are Poorly Suited to Testing Repurposed Drugs and Nutraceuticals in Cancer
The Case for Well-Conducted Observational Studies


Press Release Date May 26, 2026
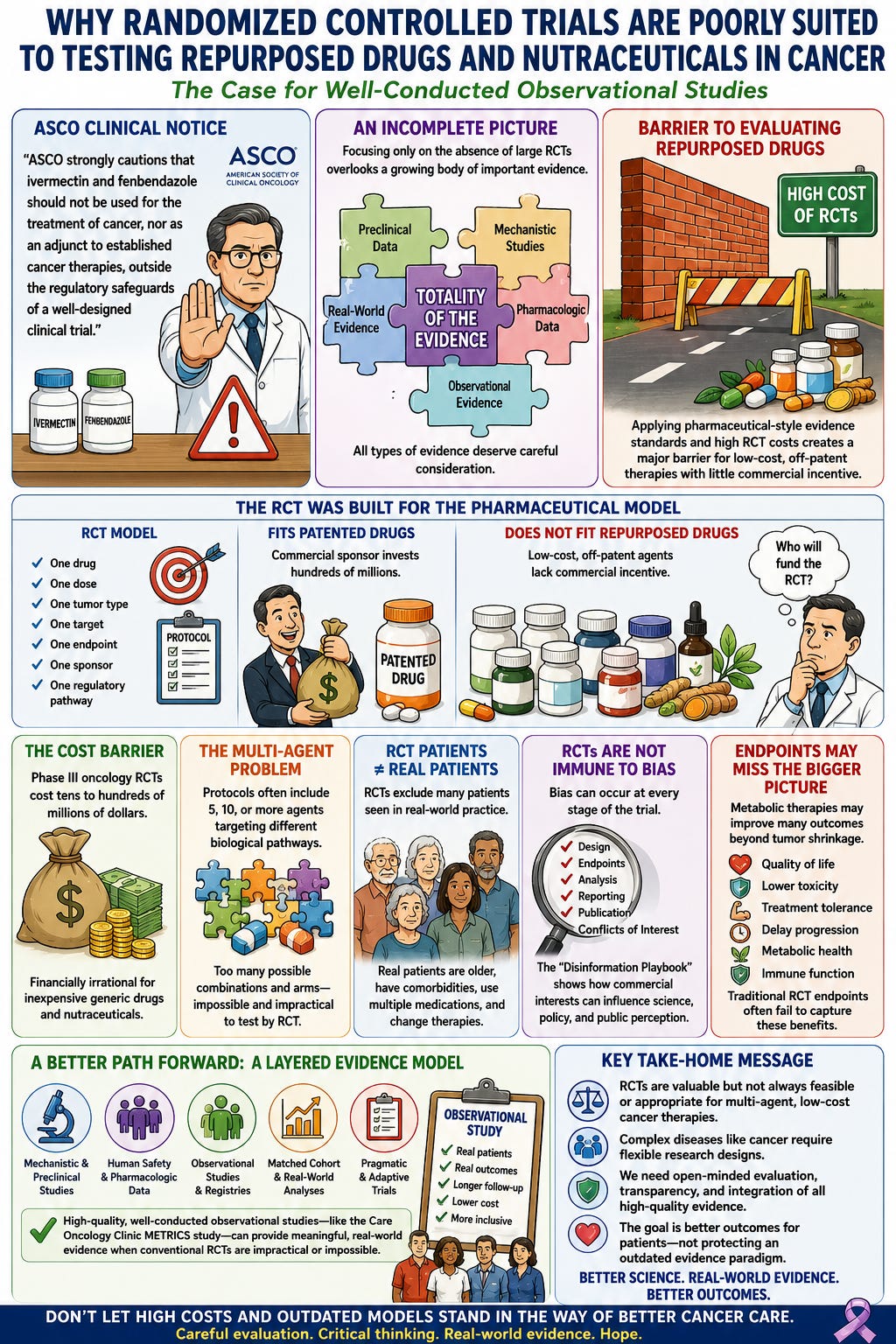
The American Society of Clinical Oncology (ASCO) Clinical Notice reflects a cautious, evidence-based position consistent with current oncology guidelines, emphasizing that neither ivermectin nor fenbendazole has been established as safe or effective for the treatment of cancer in well-conducted randomized clinical trials. This position appropriately highlights the need to consider potential toxicity, drug interactions, and the limitations of the currently available clinical evidence.
However, in my opinion, this statement presents an incomplete picture of the existing evidence and of the practical challenges involved in evaluating repurposed drugs. By focusing almost exclusively on the absence of large randomized controlled trials, it gives relatively little weight to the extensive preclinical literature, mechanistic studies, pharmacologic data, observational clinical experience, and the growing body of real-world evidence supporting further investigation of these agents.
Furthermore, applying the evidentiary standards developed for patented, single-agent pharmaceutical products to inexpensive, off-patent repurposed drugs may create a significant barrier to evaluating therapies for which there is little commercial incentive to fund the large, expensive clinical trials typically required for regulatory approval. As discussed later in this review, this raises important questions about whether the conventional evidence hierarchy is always the most appropriate framework for assessing complex, multi-agent metabolic treatment strategies.
The purpose of this review is not to claim that ivermectin or fenbendazole have been proven effective for cancer treatment (see Ivermectin and Cancer): Rather, it is to examine the totality of the available evidence, discuss its strengths and limitations, and consider whether alternative research methodologies—including well-designed prospective observational studies, pragmatic clinical trials, and carefully maintained patient registries—may provide a more practical and informative pathway for evaluating repurposed drugs in oncology.
In modern medicine, the randomized controlled trial ((RCT) has been elevated to near-sacred status. For a single patented drug tested against placebo or standard care, the RCT can be a powerful tool. It reduces bias, balances known and unknown confounders, and provides a clean estimate of the effect of one intervention under highly controlled conditions.
But cancer is not a simple disease. Nor is metabolic cancer therapy a single-drug intervention.
The emerging field of repurposed drugs and nutraceuticals in cancer is based on a fundamentally different therapeutic model. It does not ask whether one molecule can shrink a tumor by blocking one target. Instead, it asks whether a coordinated multi-agent strategy can apply simultaneous pressure across several biological domains: glucose metabolism, mitochondrial function, inflammation, angiogenesis, cancer stem cells, oxidative stress, immune suppression, and the tumor microenvironment.
This creates a profound mismatch between the intervention and the research tool. To demand a conventional RCT for every multi-drug metabolic protocol is, in practice, to demand the impossible.
The question is not whether evidence matters. It does. The question is: what kind of evidence is realistic, ethical, affordable, and clinically meaningful?
For repurposed drugs and nutraceuticals, the answer is not necessarily the traditional pharmaceutical RCT. The better answer may be carefully designed observational studies, prospective registries, matched cohort studies, pragmatic real-world analyses, and clinic-based outcomes research, such as the Care Oncology Clinic METRICS study. (1)
The RCT Was Built for the Pharmaceutical Model
The modern oncology RCT is built around a simple structure:
one drug
one dose
one tumor type
one molecular target
one primary endpoint
one sponsor
one regulatory pathway
This model fits patented pharmaceutical agents. A company develops a drug, owns the intellectual property, funds the trial, controls the protocol, selects the endpoint, recruit’s patients, analyzes the data, and submits the results for regulatory approval.
This model does not fit repurposed drugs.
Metformin, doxycycline, mebendazole, propranolol, statins, cimetidine, melatonin, vitamin D, curcumin, EGCG, sulforaphane, omega-3 fatty acids, berberine, and other agents are inexpensive, widely available, and largely off-patent. There is no obvious commercial sponsor willing to spend hundreds of millions of dollars proving that a low-cost, non-patentable combination improves survival.
This creates the central paradox: the very therapies that may be most affordable and scalable are the least likely to receive the kind of trial funding required by the conventional evidence hierarchy.
The Cost Barrier
A modern phase III oncology RCT can cost tens to hundreds of millions of dollars. Costs include trial design, regulatory approval, site activation, investigator payments, drug supply, monitoring, imaging, biomarker testing, data management, statistical analysis, insurance, and publication.
For a patented drug that may generate billions in revenue, this investment is rational.
For a protocol built from inexpensive generic drugs and nutraceuticals, it is financially irrational.
Who would fund such a trial?
Not pharmaceutical companies, because there is little profit.
Not nutraceutical companies, because they usually lack the resources and regulatory incentive.
Not government agencies, because cancer research funding is already highly competitive and often shaped by conventional therapeutic assumptions.
Not academic centers, because multi-agent metabolic protocols do not fit neatly into traditional grant categories.
The result is predictable: the absence of large RCTs is often interpreted as evidence of ineffectiveness, when in reality it may simply reflect the absence of a financial sponsor.
The Multi-Agent Problem
A second barrier is methodological.
Most metabolic oncology protocols are not single-agent interventions. They may involve 5, 10, or even 15 agents, each targeting a different biological domain.
This is not accidental. It reflects the biology of cancer.
Cancer cells are adaptive. They switch fuels, evade apoptosis, alter mitochondrial function, remodel the microenvironment, suppress immunity, activate stem-cell programs, and develop resistance. A single intervention rarely shuts down such a complex system. The logic of metabolic therapy is therefore network pressure, not single-target inhibition.
But conventional RCT design struggles with this.
If a protocol includes 10 agents, what exactly is being tested?
Each drug individually?
Each possible pair?
Each possible triple?
The full combination?
Different doses?
Different sequences?
Different rotations?
Different cancer types?
Different stages of disease?
Different background chemotherapy or immunotherapy regimens?
The number of possible trial arms quickly becomes impossible.
A 10-agent protocol cannot realistically be tested by running a separate RCT for every component and every combination. The design would be too large, too expensive, too slow, and ethically questionable.
This is one reason oncology has historically favored single-agent or two-agent trials. They are easier to regulate, easier to analyze, and easier to commercialize. But easier does not necessarily mean biologically superior.
Real Patients Are Not RCT Patients
Another problem is that RCTs often fail to reflect real clinical practice.
Patients enrolled in oncology RCTs are highly selected. They commonly have strict eligibility criteria (strict inclusion and exclusion criteria), including good performance status, adequate organ function, limited comorbidities, narrow prior-treatment histories, measurable disease, and specific laboratory parameters.
Yet real cancer patients are different.
They are older.
They have diabetes, renal impairment, cardiovascular disease, sarcopenia, cachexia, neuropathy, autoimmune disease, prior treatment toxicity, and polypharmacy.
They may use supplements, change diet, fast, exercise, or pursue integrative therapies.
They may start and stop treatments because of toxicity, cost, access, or personal preference.
In other words, real life is messy.
But metabolic oncology lives in this messy world. It is often used by patients who are between conventional therapies, recovering from toxicity, refusing further chemotherapy, trying to reduce recurrence risk, or seeking adjunctive strategies alongside standard care.
A rigid RCT may remove the very complexity that defines the intervention.
A pragmatic observational design can sometimes capture reality better than a tightly controlled RCT.
RCTs Are Not Immune to Bias
Randomized controlled trials are often regarded as the highest level of clinical evidence because they reduce selection bias and confounding. However, randomization alone cannot eliminate all sources of bias. The design, conduct, analysis, interpretation, and publication of a clinical trial remain human endeavors and are therefore susceptible to commercial, intellectual, and institutional influences.
The assumption that every randomized trial is objective, while every observational study is inherently unreliable, represents an oversimplification of the scientific process.
Industry-sponsored trials have transformed modern medicine and have produced many important therapeutic advances. Nevertheless, decades of research have shown that industry-funded studies are statistically more likely to report results favorable to the sponsor than independently funded studies. This does not necessarily imply scientific misconduct, but it does highlight the powerful influence that financial incentives can exert on every stage of the research process.
Potential sources of bias include:
Selection of comparator therapies that are inferior, outdated, or administered at suboptimal doses.
Choice of study populations most likely to demonstrate benefit while excluding patients commonly encountered in routine clinical practice.
Selection of surrogate endpoints rather than clinically meaningful outcomes such as overall survival or quality of life.
Statistical methods that emphasize favorable subgroup analyses while minimizing unfavorable findings.
Early termination of trials because of apparent benefit before long-term outcomes are established.
Selective publication of positive studies while negative or neutral trials remain unpublished.
Ghostwriting or sponsor involvement in manuscript preparation and data interpretation.
Extensive marketing of favorable findings long before independent replication has occurred.
The Disinformation Playbook published by the Union of Concerned Scientists describes a broader pattern by which commercial interests may influence the scientific literature.
Although the report examines multiple industries—including tobacco, fossil fuels, chemicals, pharmaceuticals, and food – it outlines recurring strategies that are relevant whenever substantial financial interests are involved. These include conducting or promoting biased research, manufacturing uncertainty where evidence already exists, intimidating or discrediting independent scientists, creating the appearance of independent scientific support through academic partnerships or front organizations, and influencing public policy through lobbying and regulatory pressure.
The report summarizes these recurring tactics as five components of a “disinformation playbook”:
The Fake – producing or promoting flawed or misleading science while suppressing unfavorable evidence.
The Blitz – attacking, intimidating, or discrediting researchers whose findings threaten commercial interests.
The Diversion – manufacturing uncertainty and exaggerating scientific disagreement even when substantial evidence exists.
The Screen – purchasing credibility through respected academic institutions, professional societies, or opinion leaders.
The Fix – influencing regulatory agencies or public policy to delay, weaken, or prevent actions that could threaten commercial interests.
These tactics should not be viewed as unique to any single industry or interpreted as evidence that every industry-funded study is unreliable. Rather, they serve as reminders that science operates within social and economic systems where financial incentives can influence research priorities, publication practices, and interpretation of evidence.
Oncology is particularly vulnerable to these pressures because the development of a single new anticancer drug may require investments exceeding one billion dollars and may generate revenues measured in tens of billions of dollars. Under these circumstances, commercial incentives inevitably influence which questions are studied, which therapies receive funding, and which interventions never undergo formal evaluation.
It is important to recognize that the pharmaceutical company designs the study (to achieve the result they want), conducts the study to achieve the endpoint they want, collects and manipulates the data to achieve the end-point they want, get ghost writers to write the paper and finally get the paper accepted in a top tier journal with guarantees of large indirect final compensation. Among the most influential voices in this field is John P. A. Ioannidis, whose landmark 2005 paper, Why Most Published Research Findings Are False, argued that many published conclusions may be incorrect because of a combination of methodological limitations, small sample sizes, selective reporting, multiple statistical comparisons, publication bias, and financial or academic incentives favoring positive results. (2) Richard Horton, Prior Editor-in-Chief of the Lancet, wrote in 2015 that “much of the scientific literature, perhaps half, may simply be untrue,” referring primarily to problems of study design, bias, data manipulation and reproducibility. (3)
Repurposed drugs and nutraceuticals occupy the opposite end of this spectrum. Because these agents are inexpensive, largely off-patent, and often available as generic medications or dietary supplements, there is little commercial incentive to invest the enormous sums required for conventional phase III randomized trials. Consequently, the absence of large RCTs should not automatically be interpreted as evidence that these interventions are ineffective. In many cases, it simply reflects the absence of a viable business model to finance the research.
The critical question, therefore, is not whether randomized trials are valuable—they unquestionably are—but whether they represent the only credible source of evidence for complex, low-cost, multi-agent interventions. For metabolic oncology, where therapies are individualized, adaptive, and frequently involve combinations of repurposed drugs and nutraceuticals, complementary forms of evidence—including carefully conducted prospective observational studies, pragmatic trials, registry data, and independently replicated real-world outcomes—may provide information that conventional RCTs cannot realistically generate.
The Problem of Endpoints
Conventional oncology trials often rely on endpoints such as tumor response rate, progression-free survival, or overall survival.
These are important, but they may not fully capture the value of repurposed and nutraceutical strategies.
A metabolic protocol may aim to:
slow tumor growth
reduce treatment toxicity
improve tolerance of chemotherapy
reduce inflammation
improve metabolic health
preserve muscle mass
extend time to next treatment
reduce recurrence risk
improve quality of life
delay progression
enhance immune function
support long-term disease control
Some of these outcomes are not easily captured by short-term RCTs.
For example, a low-toxicity intervention that modestly delays progression, improves metabolic health, and helps patients tolerate standard therapy may be clinically valuable even if it does not produce dramatic tumor shrinkage.
The RCT model tends to favor acute, measurable, drug-like effects. Metabolic interventions may produce slower, cumulative, system-level effects.
The Ethical Problem
There is also an ethical question.
If a patient has advanced cancer and wishes to use low-cost, low-toxicity adjunctive agents under physician supervision, is it ethical to randomize them to no such intervention for years while awaiting definitive proof?
This is especially relevant when the agents have known safety profiles, plausible mechanisms, preclinical support, epidemiologic signals, and clinical experience.
The ethical balance changes when interventions are inexpensive, generally safe, and biologically plausible.
The appropriate question becomes not, “Can we prove each agent with a billion-dollar RCT?” but rather, “Can we collect high-quality real-world evidence while protecting patients, monitoring safety, and comparing outcomes against credible controls?”
Why Observational Studies Are Better Suited
Observational studies are often dismissed as inferior. But well-designed observational research can answer questions that RCTs cannot.
For multi-agent metabolic oncology, observational studies offer several advantages.
They can include real-world patients.
They can evaluate entire protocols rather than isolated drugs.
They can follow patients over longer periods.
They can assess survival, quality of life, toxicity, treatment tolerance, metabolic markers, recurrence, and disease trajectory.
They can compare outcomes with matched historical or contemporaneous controls.
They can be conducted at far lower cost.
They can evolve as protocols improve.
They can capture patient heterogeneity rather than excluding it.
The key is rigor.
Poor observational studies are weak. But well-conducted observational studies can be highly informative, especially when they include prospective data collection, predefined endpoints, transparent protocols, appropriate comparison groups, independent statistical analysis, and adjustment for confounders.
The Care Oncology Clinic METRICS Study (1)
The Care Oncology Clinic provides an important example of this approach.
Rather than testing one patented drug, the clinic evaluated a multi-drug metabolic protocol using repurposed medications. The METRICS study represents the kind of real-world evidence framework that is more practical for this field.
Its importance is not that it provides the final answer. It does not.
Its importance is that it demonstrates a feasible research model: collect structured clinical outcomes from patients receiving a defined metabolic protocol and compare survival against expected outcomes or matched populations.
This is exactly the kind of approach that should be expanded.
Future studies should improve on this model with larger cohorts, cancer-specific registries, better matching, biomarker stratification, toxicity reporting, medication adherence data, metabolic measurements, and independent oversight.
But the direction is correct.
The Right Evidence Model for Metabolic Oncology
The future of repurposed drug and nutraceutical research should not depend on an impossible RCT standard.
Instead, it should use a layered evidence model:
mechanistic plausibility
preclinical data
human safety data
epidemiologic signals
retrospective clinical outcomes
prospective registries
matched cohort studies
pragmatic trials
adaptive platform studies
N-of-1 documentation
independent replication
This approach is more realistic and more aligned with the biology of cancer.
It also avoids the false binary that a therapy is either “proven by RCT” or “unscientific.” Science is not a single method. It is a disciplined process of observation, hypothesis, testing, replication, and refinement.
Observational evidence has always played a central role in medicine. Smoking and lung cancer were not established by randomized trials. Nor were many environmental, dietary, toxicologic, and surgical insights. In many domains, randomized trials are impractical or unethical.
Cancer metabolism may be another such domain.
The Disinformation Trap
There is one final issue.
When low-cost therapies lack large RCTs, critics often say: “There is no evidence.”
But this statement can be misleading.
Often there is evidence—mechanistic evidence, preclinical evidence, observational evidence, pharmacologic evidence, and clinical experience. What may be lacking is the specific kind of evidence that only a wealthy sponsor can usually generate.
This distinction matters.
Demanding a large RCT before even considering low-cost therapies may sound scientific, but it can function as a gatekeeping strategy. It protects the status quo, privileges patentable drugs, and marginalizes interventions that lack commercial backing.
This does not mean all repurposed drugs or nutraceuticals work. Many may not. Some may be harmful. Some may interfere with conventional therapy. Careful evaluation is essential.
But dismissing the entire field because it does not fit the pharmaceutical RCT model is not scientific skepticism. It is methodological rigidity.
A Better Path Forward
The best path forward is not to abandon evidence, but to broaden it.
For repurposed drugs and nutraceuticals in cancer, we need:
prospective patient registries
standardized protocols
clear documentation of dose and adherence
defined cancer types and stages
baseline metabolic and inflammatory markers
quality-of-life outcomes
toxicity monitoring
matched comparator groups
transparent statistical methods
independent data review
publication of both positive and negative results
This would allow the field to mature scientifically without waiting decades for trials that may never be funded.
A well-conducted observational study is not a substitute for every RCT. But in this field, it may be the most practical, ethical, and informative tool available.
It is important to note that two landmark papers published back-to-back in the New England Journal of Medicine (2000) demonstrated that well-designed observational studies can produce treatment effect estimates similar to randomized controlled trials. (4, 5) A more recent meta-epidemiologic review from the Cochrane Collaboration reached a similar overall conclusion.(6)
Conclusion
The randomized controlled trial remains an important instrument in clinical medicine. But it is not the only instrument, and it is not always the right one.
For multi-agent repurposed drug and nutraceutical protocols in cancer, conventional RCTs are often impractical, unaffordable, biologically mismatched, and poorly reflective of real-world care.
Cancer is a systems disease. A systems disease may require systems therapy. And systems therapy requires evidence models capable of studying complexity.
The Care Oncology Clinic METRICS study points toward a more realistic framework: structured, transparent, real-world observational research.
The goal should not be to lower scientific standards. The goal should be to use the right standard for the right question.
Patients with cancer do not have decades to wait for perfect trials that no one will fund.
They need honest science, transparent data, careful monitoring, and open-minded evaluation of low-cost strategies that may improve outcomes when used responsibly alongside standard care.
The future of metabolic oncology will not be built by pretending that every important question can be answered by a conventional pharmaceutical RCT.
It will be built by asking better questions, collecting better real-world data, and refusing to let commercial incentives define the boundaries of acceptable science.
At the heart of medicine is a simple principle: patient care always comes first. Every clinical decision should be guided by what is in the patient's best interests, informed by the best available evidence and individualized to the patient's unique circumstances.
References
1. Agrawal S, Vamadevan P, Mazibuko N, Bannister R, Swery R, Wilson S. A new method for ethical and efficient evidence generation for off-label medication use in oncology (A case study in glioblastoma). Front. Pharmacol. 2019;10:681.
2. Ioannidis JP. Why most published research findings are false. PLoS Med. 2005;2(8):e124.
3. Horton R. Offline: What is medicine’s 5 sigma? Lancet. 2015;385:1380.
4. Concato J, Shah N, Horwitz RI. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N Engl J Med. 2000;342(25):1887–92.
5. Benson KN, Hartz A, .J. A comparison of observational studies and randomized controlled trials. New England Journal of Medicine. 2000;342:1878–86.
6. Toews I, Anglemyer A, Nyirenda JL, Alsaid D, Balduzzi S, Grummich K, et al. Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials: a meta-epidemiological study. Cochrane Database Syst Rev. 2024;1(1):Mr000034.
If you’ve found this work valuable, please consider upgrading to a paid subscription. Your support helps me continue independent research and share practical, evolving insights—while giving you access to deeper content and more direct engagement.
New Here?
Start with the: Cancer and the Metabolic Library

Medical Disclaimer: The discussion of repurposed medications and nutraceuticals in this article is intended to review the scientific literature and does not constitute a recommendation for self-treatment. Decisions regarding the use of off-label therapies should be made in consultation with a qualified healthcare professional familiar with the patient’s medical history and current treatment plan. Please see the full Medical Disclaimer on the introductory page to Marik’s Cancer & Metabolic Healing Playbook.
Thanks..
Agree